The only non-invasive prenatal test built for more.
Unity Aneuploidy NIPT is designed not only to identify high-risk pregnancies, but also support what comes next through access to
non-invasive confirmatory testing.
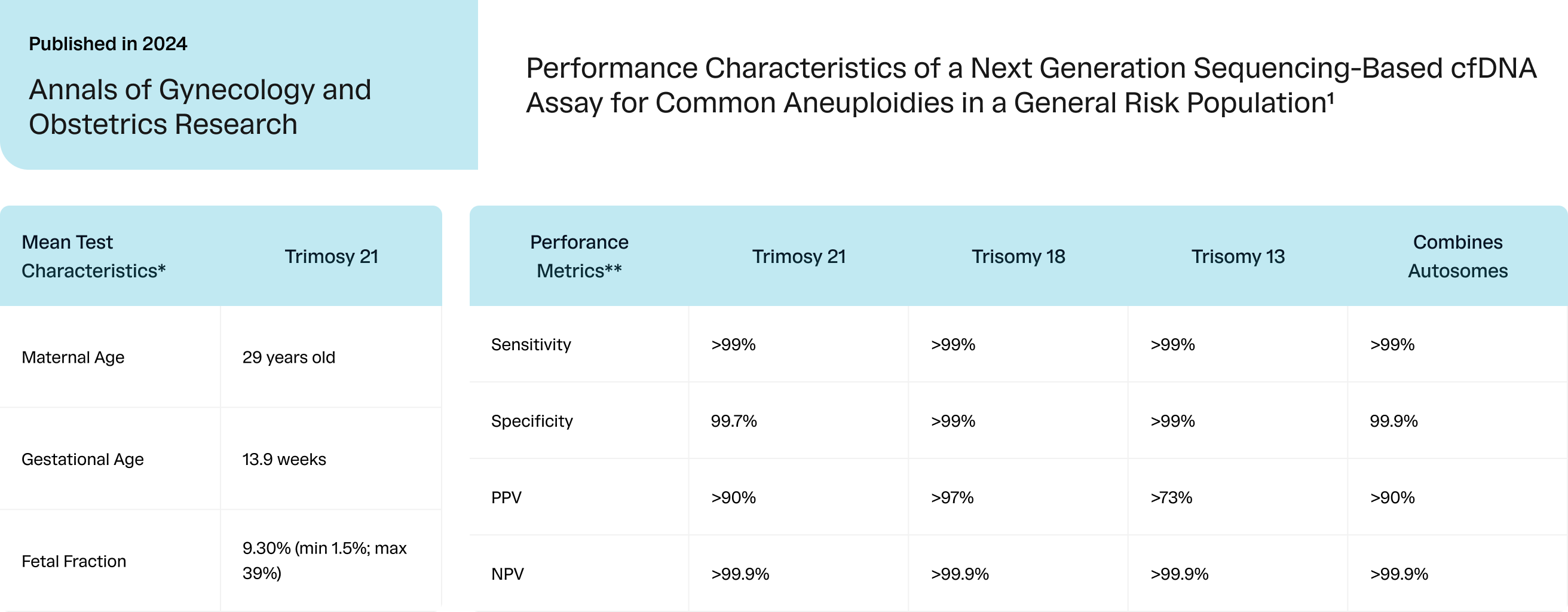
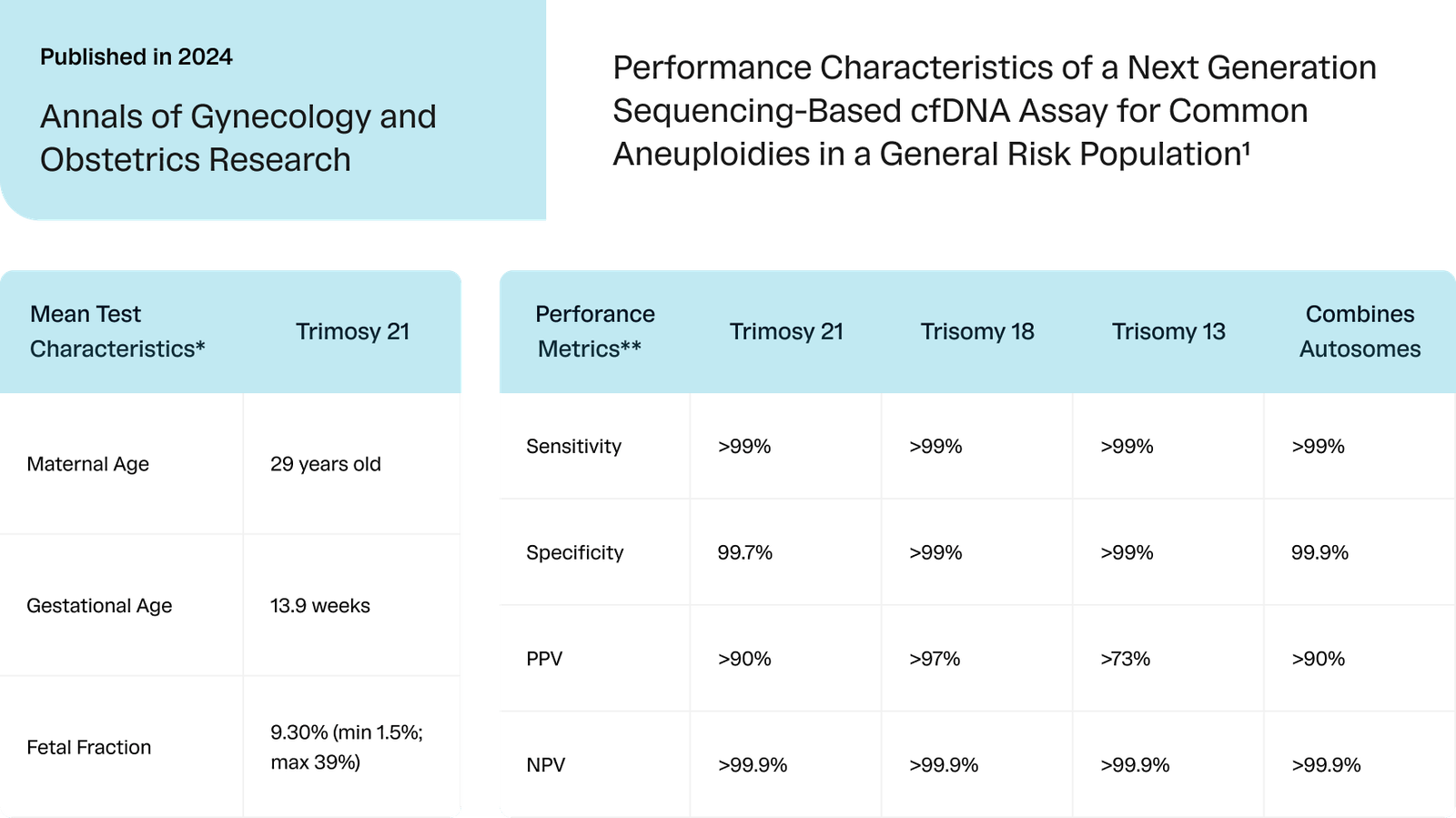
Designed as a first-line screen for the general obstetric population.1
Most NIPTs rely on a single testing method, which can result in higher no-call rates when fetal fraction (FF) is low. Unity Aneuploidy NIPT combines counting, SNP, and QCT technology with machine learning to minimize no-calls without compromising accuracy, even in the most challenging samples.
Counting
Measures relative chromosome quantity to detect deviations
The only cell-free genetic screening test that can provide a fetal risk for recessive conditions.
UNITY Fetal Risk Screen will first determine if the mother is a carrier for a recessive condition included in the test. If she is determined to be a carrier, single-gene NIPT (sgNIPT) will be performed from the same sample to determine the risk that the fetus is affected for the condition of interest. This is done via cell-free-DNA (cfDNA) and proprietary QCTTM technology. UNITY Fetal Risk Screen is the only screening test that can clarify risk down to 1 in 5,000 or up to 9 in 10 for maternal carriers.
SNPs
Calculates fetal fraction and determines zygosity
The only cell-free genetic screening test that can provide a fetal risk for recessive conditions.
UNITY Fetal Risk Screen will first determine if the mother is a carrier for a recessive condition included in the test. If she is determined to be a carrier, single-gene NIPT (sgNIPT) will be performed from the same sample to determine the risk that the fetus is affected for the condition of interest. This is done via cell-free-DNA (cfDNA) and proprietary QCTTM technology. UNITY Fetal Risk Screen is the only screening test that can clarify risk down to 1 in 5,000 or up to 9 in 10 for maternal carriers.
QCTs™ Proprietary
Enables accurate calls at low fetal fractions
The only cell-free genetic screening test that can provide a fetal risk for recessive conditions.
UNITY Fetal Risk Screen will first determine if the mother is a carrier for a recessive condition included in the test. If she is determined to be a carrier, single-gene NIPT (sgNIPT) will be performed from the same sample to determine the risk that the fetus is affected for the condition of interest. This is done via cell-free-DNA (cfDNA) and proprietary QCTTM technology. UNITY Fetal Risk Screen is the only screening test that can clarify risk down to 1 in 5,000 or up to 9 in 10 for maternal carriers.
Machine Learning
Filters noise from chromosomal correlations
The only cell-free genetic screening test that can provide a fetal risk for recessive conditions.
UNITY Fetal Risk Screen will first determine if the mother is a carrier for a recessive condition included in the test. If she is determined to be a carrier, single-gene NIPT (sgNIPT) will be performed from the same sample to determine the risk that the fetus is affected for the condition of interest. This is done via cell-free-DNA (cfDNA) and proprietary QCTTM technology. UNITY Fetal Risk Screen is the only screening test that can clarify risk down to 1 in 5,000 or up to 9 in 10 for maternal carriers.
Unity Aneuploidy NIPT is built for more.
More patients. More results. More confidence.
Unity AneuploidyTM NIPT
- Trisomy 21*
- Trisomy 18*
- Trisomy 13*
- Sex Chromosome Aneuploidies:
X, XXY, XYY, XXX - Zygosity
- 22q11.2 Microdeletion Syndrome*
- Fetal Sex*
Unity Fetal AntigenTM Tests
- Big C, little c, D, E, e, Fya (Duffy), Fyb (Duffy), jka (Kidd), jkb (Kidd), K (Kell), k, M, N, Big S, little s, U
- *M and N antigens must be selected at ordering and cannot be added after the test is submitted
- HPA-1a (with HLA-DRB3*01:01 when applicable), HPA-1b, HPA-2a, HPA-2b, HPA-3a, HPA-3b, HPA-4a, HPA-4b, HPA-5a, HPA-5b, HPA-9a, HPA-9b, HPA-15a, HPA-15b
Unity ConfirmTM
Non-invasive confirmatory testing for patients who receive high-risk Unity Aneuploidy NIPT results.*
Powered by Fetal Cell Capture™ technology, Unity Confirm uses whole genome sequencing of intact circulating fetal cells.
Only with Unity Aneuploidy NIPT
Where screening ends, something new begins.
Although amniocentesis remains the gold standard, many patients cannot, choose not to, or are still considering whether to pursue invasive diagnostic testing after a high-risk Aneuploidy NIPT result.2,3,4
Powered by Fetal Cell Capture™ technology, Unity Confirm captures intact circulating fetal cells – delivering rapid CVS-like insights – without the procedural risks.*
Only with Unity Confirm

Non-invasive confirmatory testing
Accessible following a high-risk Unity Aneuploidy Screen result through 15 weeks 6 days gestation**
Whole genome sequencing of individual intact circulating fetal cells
Effectively provides 100% fetal fraction***
Imaging and sequencing-based fetal cell confirmation allowing for high accuracy
* Unity Confirm and rapid CVS both analyze fetal-derived trophoblast cells. Unity Confirm isolates individual cells via whole genome sequencing, which is performed on each cell separately, whereas rapid CVS is often performed via FISH. While rapid CVS may analyze more cells, WGS generates more data per cell. In both rapid CVS and fetal cell capture, mosaicism cannot be excluded. No medical decisions should be made based on Unity Confirm alone. Clinical correlation is necessary.
** Unity Confirm is not available for high-risk monosomy X pregnancies, twin or higher multiple pregnancies, vanishing twins, gestational carriers or egg donors, or for pregnancies >15 weeks 6 days gestation. Only available in the US.
*** In rare instances, results may rely on a single cell that is co-sequenced with 1-2 maternal cells, which may reduce fetal fraction to 33% or 50%. When this occurs, the report clearly indicates this limitation.
Unity Fetal Antigen™ Tests
Available exclusively through Unity Aneuploidy NIPT. Comprehensive fetal antigen testing for when clinical needs arise.
Additional Provider Resources.

Unity Aneuploidy NIPT Brochure

Test Requisition Form
Unity Confirm Brochure
Innovation with Unity does not stop here.
When you choose Unity, you are partnering with a company committed to advancing prenatal care and redefining how patients and providers navigate prenatal testing. Request a test kit for your clinic today to streamline access and elevate patient care.
Unity tests can produce false-positive and false-negative results. Results are not a guarantee. Amniocentesis should always be considered with high risk results. Important medical decisions should not rely on Unity test results alone. Clinical correlation is necessary, including but not limited to the results of prior and further prenatal testing. Unity tests are laboratory-developed tests performed in a CLIA-certified and CAP-accredited laboratory. They are not FDA-approved or FDA-cleared diagnostic tests. Test performance may vary based on gestational age and other factors.
References
Wynn, J., et al. “Performance Characteristics of a Next Generation Sequencing-Based cfDNA Assay for Common Aneuploidies in a General Risk Population.” Ann Gynecol Obstetr Res. 2024; 7 (1) 1027
Okoror, Collins Ejakhianghe Maximilian, and Suruchi Arora. “Prenatal diagnosis after high chance non-invasive prenatal testing for trisomies 21, 18 and 13, chorionic villus sampling or amniocentesis?–Experience at a district general hospital in the United Kingdom.” European Journal of Obstetrics & Gynecology and Reproductive Biology: X 19 (2023): 100211.
Mokhtar, Rifat, et al. “Comparing noninvasive prenatal testing with invasive testing for the detection of trisomy 21.” Cureus 14.11 (2022).
Chetty, Shilpa, Matthew J. Garabedian, and Mary E. Norton. “Uptake of noninvasive prenatal testing (NIPT) in women following positive aneuploidy screening.” Prenatal Diagnosis 33.6 (2013): 542-546.
Singleton, B. (2000). The presence of an RHD pseudogene containing a 37 base pair duplication and a nonsense mutation in Africans with the Rh D-negative blood group phenotype. Blood, 95(1), 12–18. https://doi.org/10.1182.
Zhang J, et al. RHD Genotypes in a Chinese Cohort of Pregnant Women. Front Genet. 2021 Dec 14;12:752485. doi: 10.3389/fgene.2021.752485. PMID: 34970297; PMCID: PMC8712876.